
ASNC is your source for the latest information emerging from the field of nuclear cardiology and cardiac imaging.
From our flagship scientific journal to our weekly newsletter, ASNC is dedicated to delivering high-quality research, news, and updates from the field.
ASNC News
The ASNC media team is available to arrange interviews with experts on the news featured in ASNC’s press releases, on research published in the Journal of Nuclear Cardiology, and on other developments in nuclear cardiology.
-
Investing in Innovation: ASNC Announces Recipients of New Research Grants
June 8, 2026 -

Dr. Mouaz Al-Mallah Will Present the Mario Verani Memorial Lecture at ASNC2026 in Las Vegas
May 7, 2026 -
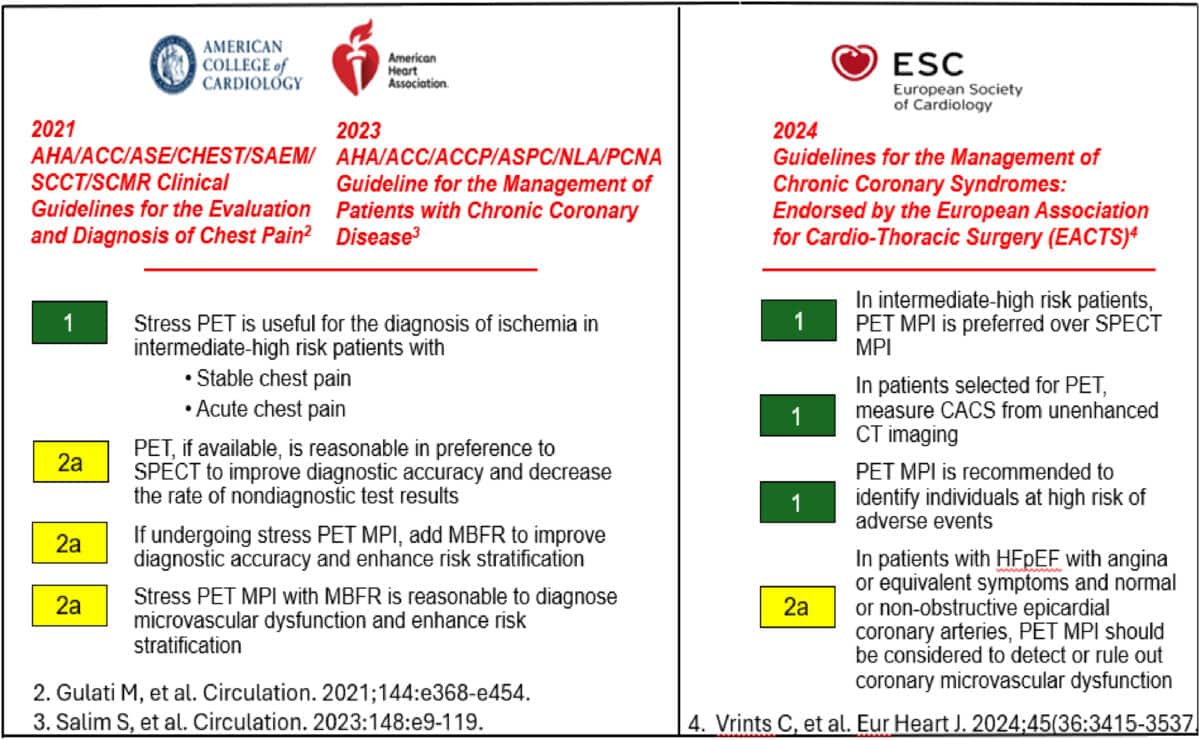
Cardiac PET with Myocardial Blood Flow Is Now the Preferred Test for Evaluating Coronary Artery Disease in All Patients
January 26, 2026 -
Jamieson M. Bourque, MD, MHS, FASNC, Installed as 2026 President of the American Society of Nuclear Cardiology
January 6, 2026

Journal of Nuclear Cardiology
The Journal of Nuclear Cardiology (JNC) is the only journal in the world devoted to this dynamic and growing subspecialty. The JNC is the official peer-reviewed publication of ASNC featuring the latest research findings and clinical developments in nuclear cardiology and related fields.

Latest Journal Issue
Read the latest issue of the Journal of Nuclear Cardiology (JNC). Full access to the JNC is available with an ASNC Membership. Join or renew today!
New JNC Podcast
The JNC CardioConnect podcast links experts, insights, and innovations in nuclear cardiology. Join Editor-in-Chief Marcelo F. Di Carli, MD, MASNC, and authors as they discuss important articles from the Journal of Nuclear Cardiology (JNC).
ASNC Updates
Access the latest news and updates from ASNC. Search by category of interest, date, and more.

House Subcommittee Advances Prior Authorization Legislation
The House of Representatives Energy and Commerce Subcommittee on Health has advanced…
Lawmakers Seek to Halt Medicare’s AI-Assisted Prior Authorization Model
The House of Representatives Appropriations Committee has approved legislation that, if passed,…
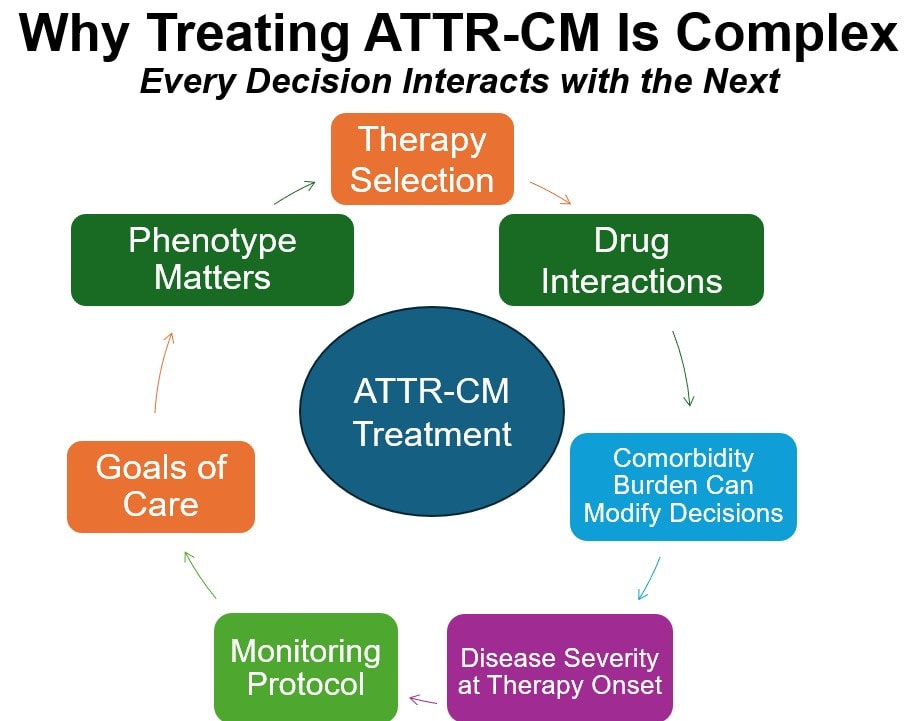
Diagnosis Confirmed! What to Do Next for Your ATTR-CM Patients
Last week, ASNC welcomed clinicians from around the world to Confirming the…
Receive ASNC Newsletters
Flashpoint
ASNC members receive the Society’s weekly newsletter that includes training and credentialing news, legislative and regulatory updates, international news, meeting and program information, and more.
ASNC SmartBrief
Sign up to receive a complimentary bi-weekly newsletter featuring the latest news, trends, and insights shaping the nuclear cardiology community. Stay informed with a curated roundup of top stories and updates from leading sources.
ASNC Interview Series
Explore the latest topics in nuclear cardiology through video conversations with luminaries and key leaders in the field.
ASNC Imaging Insights
Imaging Insights is a feature publication with in-depth articles that provide a deeper look at important developments and news in nuclear cardiology.
")

Advertise with ASNC
ASNC is where your marketing investment reaches the right audience and achieves optimal return.
